Case Study: Connecting with Patients through Blood Pressure
Remote BP monitoring – Self Monitoring Blood Pressure (SMBP) improves outcomes at Excel Medical Center Practices
A new remote blood pressure monitoring protocol – Self Monitoring Blood Pressure (SMBP) is leading to unprecedented outcomes for patients at the Excel Medical Center practices. By combining patient-measured blood pressure and nurse-led remote check-ins with resources and collaboration from the American Heart Association’s Target:BP program and the Frazier Family Coalition for Stroke Education and Prevention program, the Excel practices have achieved blood pressure control levels of up to 89%.
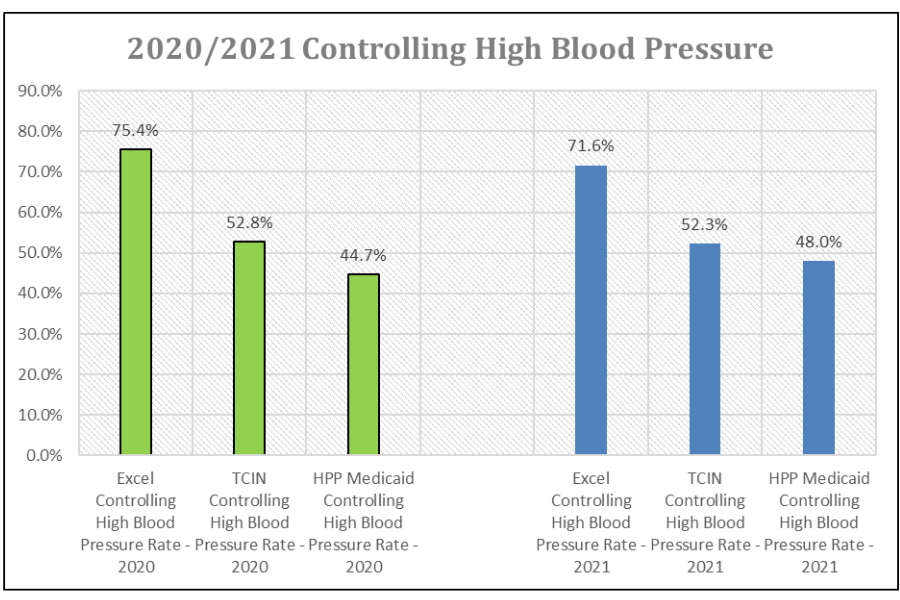
The attributed EXCEL Medical practices achieved a performance rate of 71.6% in the target HEDIS measure, “controlling blood pressure” for the covered year 2021 with one practice performing at 89.9%. EXCEL performed better than the Health Partners Plan overall average performance of 48.05%.
How It Works
Intervention Summary
The Self-Monitoring Blood Pressure (SMBP) team reaches out to enroll their high-risk patients with uncontrolled BP (systolic >140 or diastolic >90); excessive hospital emergency department and hospital admission utilization due to uncontrolled high blood pressure. The patients are provided with a blue tooth BP monitoring medical equipment for home.
The practice based nurse practitioner provides patient education and support materials provided by the American Heart Association with their logos and the EXCEL Medical, LLClogo in 3.
The SMBP team checks in regularly and when triggered by patient alerts to provide case management and patient support.
The SMBP team circles back to the patient’s primary care provider to discuss patient issues, follow up, medication adjustments, if needed and to integrate care.
The patients are also referred to the Frazier Coalition for Stroke Education and Prevention Enrollment into the 6 months Hypertension Self-Management and Educational Support Program.
Personnel Involved
- Excel nurse practitioner
- Two Excel medical assistants
- Excel primary care physicians Temple Center for Population Health, Director Temple Care Integrated Network
Primary Outcomes
- Collectively, the attributed TCIN EXCEL Medical practices achieved a performance rate of 71.6% in the target HEDIS measure, “controlling blood pressure” for the covered year 2021. They performed better than the Health Partners Plan overall average performance of 48.05%.
- The top three Excel Medical practices which performed the best and the highest of all the attributed TCIN practices in both Tier 1 and Tier 2 in the HEDIS measure “controlling blood pressure” were:
- 1216 North Broad Street – this EXCEL Medical practice performed at 89.9% rate which is the highest performance of all the attributed TCIN practices in the CBP HEDIS measure.
- 2724 N. 5th Street – EXCEL Medical practice performed at 78.95% rate which is the 2nd highest performance of all the attributed TCIN practices in the CBP HEDIS measure.
- 521 W. Girard Avenue - EXCEL Medical practice performed at 77.4% rate in the CBP HEDIS measure and the 3rd highest performance of all the attributed TCIN practice in the CBP HEDIS measure
- These three EXCEL Medical practices which performed the best in the HEDIS CBP measure all all enrolled in the EXCEL SMBP program.
- All of the seven (7) attributed TCIN EXCEL Medical practices, which include the practices that currently participate in the SMBP program earned incentive payments for achieving the HEDIS measure, “controlling blood pressure” targets for covered year 2021.
- In conclusion, overall the TCIN practices, Tier 1 and Tier 2 performed better in the HEDIS measure “CBP” at a rate of 52.31% than the Health Partners Plan overall average performance of 48.05%.
Although blood pressure is just one metric, it was giving us a bigger picture of what was happening to our patients. Some of these patients got really excited, and they would come in and tell us, ‘My blood pressure’s been good.’ The payoff is that they are invested.

Q&A
We asked three Temple and Excel Medical Center personnel to share their experiences setting up and implementing the remote blood pressure monitoring program:
- Vanessa Exama-Molin, AGPCNP (Excel Medical);
- Theodore Burden, MD, MBA (Excel Medical); and
- Chevonne DaSilvio-Nash, MBA, HCA (Temple Center for Population Health)
The following are excerpts from our conversation.
Exama-Molin: I’m a nurse practitioner who manages the remote program with two medical assistants who receive and check all blood pressure alerts on a daily basis. I set parameters so they know what to do based off the reading they see. For example, if a patient has a systolic BP of 160–170, they’re supposed to call the patient as soon as they receive that alert, have them re-check it, ask whether they took their medications, whether they are having symptoms of chest pain, headache, etc., and use that information to determine next steps such as referrals or medication adjustments.
Exama-Molin: Our internal remote patient monitoring program started around December of 2020. We identified those patients in our practice who were not meeting our blood pressure goals of systolic of 140 or less, or diastolic of 90 or less. Once identified, we started supplying them with blood pressure machines to check at home. My team began monitoring remotely and it took off very quickly. In March or April of 2021, Chevonne from the Temple Center for Population Health contacted Excel to discuss the Frazier Family Collation and the AHA Target:BP program. Because we already had a remote patient monitoring program implemented, we put our heads together. They set up everything on the back end and all the programs came together.
The AHA Target BP program requires monitoring of blood pressure from our end. They also provided us with patient resources—videos, pamphlets—in both Spanish and English. They taught patients how to take their blood pressure properly, types of foods to eat, what systolic and diastolic mean, signs and symptoms to watch out for. Target BP really amplified the resources available to help our patients manage their blood pressure. All of our patients showed great appreciation for it.
Exama-Molin: Initially, the patients were somewhat irritated. If they have not used the device, we’re calling them; if their blood pressure reading is past the parameter that we’ve set, they’ve receiving a call. Some of them might receive a call two or three times a day. But after you have the same medical assistant calling them for two or three months, some of them would open up. We had a patient who had multiple deaths in the family during the pandemic, and that was contributing to the stress of their blood pressure being uncontrolled. So now the medical assistant was not just saying, “Did you take your medication?” They’re saying, “How’s everything else around you going?” Patients see that you’re invested in them, so why wouldn’t I invest in myself? That’s how we really got them to be excited. The model of the program is what helps you to get those patients invested.
Burden: From the practitioner’s side we didn’t have to set up much because Vanessa monitored the patients for us. But keep in mind that blood pressure’s just one metric—these patients have got a lot going on. It seemed to me to be a little disjointed just taking blood pressure out of the day-to-day equation. We thought our providers should take a more active role in the process so they could do the clinical management. We thought, let’s get these patients plugged back in to the providers.
Exama-Molin: How we did that was, as the provider in charge of overseeing the patients within the blood pressure program, if I made any medication adjustments, or I reached out to a patient’s cardiologist, for example, I would then text, call, or internally message their provider, just to bring everything together.
The PCPs actually enjoy and appreciate it. They are aware if I’ve made a change or a recommendation, and it shows the patient that the practice as a whole is working together and is invested in their blood pressure.
DaSilvio-Nash: All seven Excel practices that were in the TCIN network at the start of covered year 2021 (an additional practice was added mid-year as the EXCEL Medical, LLC acquired an existing TCIN attributed practice) performed very well with controlling high blood pressure. The average performance for BP control among Health Partners Plan members across all networks was 48.05%; TCIN practices overall were at 52.31%. The three top-performing Excel practices performed at 89.19%,, 78.95%, and 77.4%. (the highest of all TCIN practices). All Excel practices performed over 50%, and 5% higher than the plan which is the metric for meeting HEDIS payment incentive requirements.
Exama-Molin: We’ve noticed that when the patients are coming to the office, they’re happier about their blood pressure. We’re still educating them, but not really harping on them, because they are doing better. Now we’re congratulating them.
I have also seen a lot of the patients that were very uncontrolled, they would go to the ER quite a lot, for a [systolic] blood pressure that’s 170 or 180 and it’s really that they were non-adherent. Now they’re not going to the ER so much, they’re coming to their regular visits with me and they’re thriving.
DaSilvio-Nash: Practice operations considerations are definitely important when planning to develop and implement a SMBP program in the practice. The practice infrastructure and available resources such as staffing, staff training, and budgeting, to name a few are things to consider when developing a successful SMBP program.
For example:
- Available staffing to support and manage the workflow of the SMBP program. There are several operational workflow components that need to be developed in order to successfully manage a SMBP program.
- Access to available US Validated blue tooth blood pressure cuff devices that are compatible and data integration.
- Accessibility of Data and I.T. Technology
- Blue tooth enabled self-reporting ability
- Electronic medical record integration with vendor neutral-smartphone app
- Cellular Data Transmission Options
Funding for a SMBP program is also something to consider. Some of the TCIN practices have received grant funding via the HRSA Hypertension Initiative which provide funding to health centers to support those centers that could benefit from assistance to help their patients diagnosed with hypertension control and improve their blood pressure outcomes.
Other practices, such as EXCEL Medical have used their own funds to support a SMBP program in the practices Therefore, partnering with the American Heart Association (AHA) is a really good opportunity for the practices to have access to patient educational and support resources, best practice publications, loaner devices such as eligible Bluetooth blood pressure cuffs that are interchangeable through the practice EMR system, and downloadable tools to assist the practice with implementing a SMBP program and Target:BP
Burden: That’s extremely important from the practice standpoint, the logistics. Hospitals have the resources to be able to pay for those things; private practices don’t. So cost-efficiency needs to be factored in.
Burden: We had this process set up before our involvement with Frazier/AHA, but as we joined other relationships, we realized the potential was greater than what we were trying to do by ourselves. The blood pressure metric was giving us a bigger picture of what was happening to our patients—not only on their blood pressure but on everything else they were doing. Some of these patients got really excited about following their blood pressure and doing the kinds of things that they should be doing, and they would come in and tell us, “My blood pressure’s been good!” Or, “Dr. Burden, the problem is my blood pressure.” The big picture is to make sure that they are invested.
DaSilvio-Nash: The TCIN is committed to working as a team to improve care coordination and the delivery of effective patient-focused care. Educating our patients on disease management supports better patient engagement, encourages healthy lifestyle change, and reduces length of stay and readmission rates and cost. It’s important that we identify those uncontrolled diagnoses, like hypertension, that are driving increased hospital admissions and readmissions to improve the health outcomes for our patients.
Also In This Issue
- Beating the Odds in Hypertension Management
By Steven R. Carson, MHA, BSN, RN - Educational Video Resources from Temple Specialists
View Now - Setting Up Self-Monitored Blood Pressure (SMBP) for Empowered Care
Learn best practices for implementing self-measured blood pressure through the AHA Target: BP program. - Get Support Through Target: BP™
Find out how to enroll in the AHA/American Medical Association Target BP program.
Learn More - Resources for Providers and Patients
Access resources for providers and patients to improve hypertension management.
